If you have been dealing with progressively heavier periods, increasingly severe cramps, and a doctor who tells you your uterus looks "bulky" or "enlarged" — adenomyosis may be at the root of it. It is a condition that affects a significant number of women in their reproductive years, yet it remains poorly understood, frequently dismissed, and consistently underdiagnosed. Many women spend years cycling through treatments that address their symptoms without anyone identifying the underlying cause.
I want to give you a thorough, honest picture of what adenomyosis actually is, what causes it, how it is diagnosed, and what a genuinely comprehensive management strategy looks like — one that includes natural and lifestyle interventions alongside the appropriate medical options.
What Adenomyosis Actually Is
Adenomyosis is a condition in which tissue similar to the uterine lining — the endometrium — grows into the muscular wall of the uterus, known as the myometrium. That is the key distinction: the tissue is growing into the uterine wall, not outside the uterus. Think of it like a thick, saturated sponge embedded within the uterine muscle itself.
This displaced tissue behaves just like the endometrial lining does during a normal cycle: it thickens and engorges in response to estrogen, then breaks down and bleeds with each period. But because it is trapped inside the muscular wall with nowhere to shed, this process creates intense pressure, inflammation, and abnormal uterine contractions — which is why the pain and bleeding associated with adenomyosis can be so severe.
Over time, as the tissue continues to grow into the myometrium, the uterine walls thicken and the uterus itself becomes enlarged. This is what doctors mean when they describe a "bulky uterus" — a phrase women with adenomyosis hear frequently, often without a clear explanation of what is causing it or what it means for their health.
How Adenomyosis Differs from Endometriosis
Adenomyosis and endometriosis are related conditions — they both involve endometrial-like tissue growing where it does not belong — but they are not the same thing, and this distinction matters for both diagnosis and management.
In endometriosis, the endometrial-like tissue grows outside the uterus: on the fallopian tubes, ovaries, peritoneum, bowel, bladder, and in rare cases even further afield. In adenomyosis, the tissue grows into the uterine wall itself. One condition is about invasion outward; the other is about invasion inward.
Importantly, these two conditions frequently co-occur. Research suggests that approximately 20 percent of women with endometriosis also have adenomyosis. If you have endometriosis, adenomyosis is worth investigating — especially if your bleeding is heavier or your cramps are worse than endometriosis alone would typically explain. The reverse is also true: if you have adenomyosis and your pain seems disproportionate to what imaging shows, endometriosis may also be present.
Symptoms: What Adenomyosis Actually Feels Like
Symptoms of adenomyosis tend to worsen progressively over time, and they often intensify in the years approaching perimenopause as estrogen levels fluctuate more dramatically. Up to a third of women with adenomyosis are completely asymptomatic — the condition is found incidentally. For those who do have symptoms, the picture typically includes:
- Extremely heavy bleeding: This is driven by two factors — an increased surface area of the endometrium (because the tissue has invaded further into the uterine wall) and increased vascularization of the uterine lining. The result is heavy periods that can involve large clots, flooding, and bleeding that soaks through protection within an hour.
- Severe cramping and menstrual pain: Abnormal uterine contractions caused by the embedded tissue, combined with elevated levels of pro-inflammatory prostaglandins and eicosanoids, create cramping that can be genuinely debilitating.
- Painful sex (dyspareunia): Particularly deep, aching pain during intercourse — caused by the enlarged, tender uterus and surrounding inflammation.
- Pelvic pressure and bloating: As the uterus enlarges, many women experience a persistent sense of fullness, heaviness, or pressure in the lower pelvis.
- An enlarged or tender uterus: The uterus may be palpably enlarged on exam — sometimes two to three times its normal size in severe cases.
- Spotting between periods: Abnormal uterine bleeding, including intermenstrual spotting and large clots, is common.
- Worsening symptoms with age: Unlike many cycle-related conditions that fluctuate, adenomyosis symptoms typically intensify as women move through their 30s and into their 40s — because the longer the estrogen-driven tissue has to grow, the more embedded it becomes. Symptoms generally resolve after menopause.
The Diagnosis Challenge
Adenomyosis has historically been one of the most underdiagnosed conditions in women's health — and there is a structural reason for that. For most of medical history, a definitive diagnosis could only be made by examining uterine tissue after a hysterectomy. You can imagine how many cases were never identified under that system.
Modern imaging has improved the picture somewhat, but it is still far from straightforward:
- Transvaginal ultrasound can suggest adenomyosis — particularly three-dimensional transvaginal ultrasound, which is significantly more sensitive than the standard two-dimensional version and can detect the condition at an earlier stage. But ultrasound findings are not definitive, and a normal-appearing ultrasound does not rule out adenomyosis.
- MRI is the most accurate non-invasive imaging tool for adenomyosis. It can visualize the thickened junction zone between the endometrium and myometrium and identify areas of adenomyotic invasion. However, MRI is not always accessible, and many practitioners do not think to order it.
- Definitive histological diagnosis still technically requires examination of uterine tissue — which in practice means either hysterectomy or, in some cases, biopsy during surgery. This is one reason adenomyosis continues to be diagnosed far later than it should be, and why the diagnostic burden often falls on the woman to advocate persistently for herself.
Adenomyosis disproportionately affects Black women compared to women of other races, and it is most commonly diagnosed in women in their 30s and early 40s — often because this is when symptoms become severe enough to seek answers, or when fertility challenges prompt closer investigation. Women who have been pregnant or had uterine surgery (including cesarean sections) appear to be at higher risk, possibly because those events create opportunities for endometrial tissue to infiltrate the myometrium.
Root Causes: What Drives Adenomyosis
Research into adenomyosis is still developing — it has received far less attention than conditions like endometriosis. What the available evidence points to is a convergence of several overlapping mechanisms.
Estrogen dominance and local hyperestrogenism
Adenomyosis is an estrogen-driven condition. The adenomyotic tissue tends to have a higher number of estrogen receptors than normal endometrial tissue and an increased sensitivity to estrogen, creating a state of localized hyperestrogenism within the uterus. Anything that contributes to estrogen dominance systemically — insufficient progesterone, impaired estrogen clearance, gut dysbiosis, liver overload — feeds this local estrogen environment and drives the growth and activity of adenomyotic tissue. Perimenopause, with its pattern of erratic and often elevated estrogen relative to progesterone, is a well-recognized driver of symptom escalation.
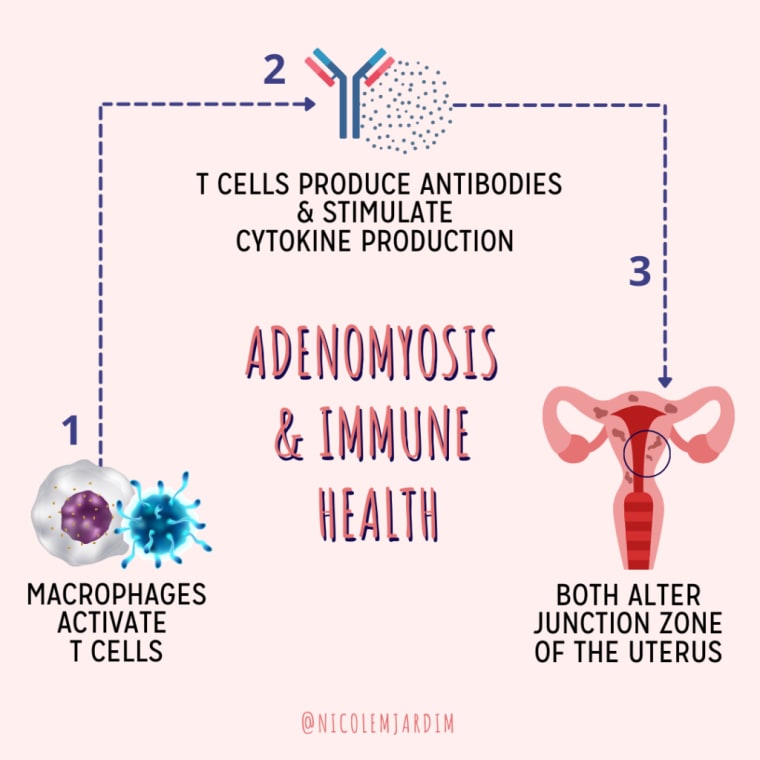
Immune system dysfunction and inflammation
Like endometriosis, adenomyosis appears to involve altered immune function in the uterus. Research shows that women with adenomyosis exhibit changes at the junction zone — the boundary between the endometrium and myometrium — driven in part by macrophage activity and abnormal cytokine production. The immune system's failure to recognize and clear the invading tissue, combined with the chronic inflammatory response it generates, creates a self-reinforcing cycle that deepens the invasion over time. Elevated pro-inflammatory prostaglandins and eicosanoids produced by this immune response directly drive the pain and abnormal contractions characteristic of adenomyosis.
Genetic predisposition
There is evidence of a genetic component to adenomyosis, similar to what is seen with endometriosis. Women with close relatives who have the condition are at elevated risk. Genes appear to influence estrogen receptor sensitivity, immune regulation, and the behavior of endometrial cells — all of which are relevant to adenomyosis development. As with most conditions, genetics are not destiny, but they are part of the picture.
Uterine injury history
Prior uterine surgery or trauma — including cesarean sections, uterine rupture during pregnancy, dilation and curettage (D&C) procedures, and myomectomy — appears to increase adenomyosis risk. The working hypothesis is that disruption to the endometrial-myometrial boundary creates pathways through which endometrial tissue can infiltrate the muscular wall. This does not mean that having a cesarean section or D&C causes adenomyosis, but it is a relevant risk factor worth knowing about.
The Natural Protocol: What Can Actually Help
Before going into specifics: natural approaches to adenomyosis can meaningfully reduce symptoms, lower systemic and uterine inflammation, support hormonal balance, and significantly improve quality of life. They do not, however, remove adenomyotic tissue or reverse the structural changes in the uterine wall that have already occurred. Think of the natural protocol as essential management — it addresses the hormonal and inflammatory environment that is driving the condition, reduces symptoms, and supports overall wellbeing while you pursue whatever medical approach is appropriate for your situation.
Anti-inflammatory nutrition
Diet is one of the most powerful tools available for managing adenomyosis, because it directly targets the inflammatory and estrogenic drivers of the condition. The core priorities are:
- Reduce the major inflammatory drivers: Gluten, conventional dairy, refined sugar, alcohol, and processed vegetable oils are the primary dietary contributors to the systemic inflammation that feeds adenomyosis. Reducing or eliminating these — even temporarily — often produces noticeable improvements in bleeding and pain within two to three cycles.
- Emphasize omega-3 fatty acids: Fatty fish (salmon, sardines, mackerel), flaxseeds, chia seeds, and walnuts provide EPA and DHA, which directly counter the prostaglandin-driven inflammation responsible for cramping and heavy flow. A high omega-3 to omega-6 ratio in the diet is one of the most impactful shifts you can make for period pain.
- Load up on colorful vegetables: Deeply colored vegetables — particularly leafy greens, beets, berries, and orange and red produce — are rich in antioxidants that combat the oxidative stress driving uterine inflammation.
- Cruciferous vegetables for estrogen metabolism: Broccoli, kale, Brussels sprouts, cabbage, and cauliflower contain indole-3-carbinol (I3C) and diindolylmethane (DIM), which support the liver's ability to metabolize estrogen down the less inflammatory 2-OH pathway. Aim for one to two servings daily.
- Prioritize fiber for estrogen excretion: Adequate fiber (25–35 g daily) binds estrogen in the gut so it is excreted rather than reabsorbed. Legumes, seeds, vegetables, and whole grains all contribute.
Estrogen dominance support
Because adenomyosis is driven by a hyperestrogenic uterine environment, actively supporting estrogen clearance is essential. This works on two fronts: supporting the liver's ability to break down estrogen, and ensuring that processed estrogen is excreted rather than recirculated via the gut.
- DIM (diindolylmethane): A compound derived from cruciferous vegetables that supports phase 1 of liver estrogen detoxification and encourages metabolism down the less estrogenic 2-OH pathway. DIM is particularly useful when estrogen is elevated and phase 1 liver detox needs support. It can be obtained through concentrated cruciferous vegetable intake or as a targeted supplement.
- Liver support: Milk thistle, dandelion root, artichoke extract, and N-acetyl cysteine (NAC) all support the liver's ability to process and clear estrogen. A well-functioning liver is critical for keeping estrogen levels in check.
- Daily bowel movements: Constipation means estrogen that the liver has processed and sent to the gut for excretion gets reabsorbed instead. Fiber, adequate hydration, magnesium, and movement are all key to keeping transit time optimal.
- Blood sugar stability: Blood sugar dysregulation elevates insulin, which amplifies estrogen production and inflammation. Stable blood sugar — through balanced meals with adequate protein and fat, and minimizing refined carbohydrates — is foundational.
Progesterone support to balance estrogen
Adequate progesterone is the natural counterbalance to estrogen's proliferative effects on uterine tissue. Progesterone is only produced in meaningful amounts after ovulation — which means ensuring you are ovulating consistently, and that the quality of ovulation is good, is essential. Chronic stress, poor blood sugar regulation, undereating, and thyroid dysfunction all impair ovulation and therefore progesterone production. Addressing these foundational issues is the primary approach. Some women benefit from additional support via Vitex (chasteberry), which can support the LH surge and luteal phase progesterone production, or in appropriate cases, bioidentical progesterone cream used in the luteal phase — ideally in consultation with a knowledgeable practitioner.
Castor oil packs for pelvic pain
Regular use of castor oil packs over the lower abdomen is one of the most consistently beneficial therapies for adenomyosis-related pelvic pain and uterine inflammation. Castor oil is rich in ricinoleic acid, which has anti-inflammatory and analgesic properties. Applied topically with gentle warmth, it stimulates lymphatic flow, increases circulation to the pelvic organs, supports detoxification, and reduces the uterine congestion that drives pelvic pressure and pain. Women with adenomyosis report meaningful reductions in cramping, bloating, and pelvic heaviness with regular use. Apply to the lower abdomen for 30–60 minutes, three to four times per week. Avoid during menstruation and during the luteal phase if you are actively trying to conceive.
Targeted supplements
Several supplements have specific evidence or strong clinical rationale for adenomyosis management:
- NAC (N-acetyl cysteine): One of the most important supplements for conditions involving endometrial-like tissue. NAC reduces oxidative stress, supports glutathione production — the body's master antioxidant — and directly targets the chronic inflammation driving adenomyotic tissue activity. It also supports liver detoxification and estrogen clearance. A commonly used dose is 600 mg twice to three times daily.
- Magnesium: Magnesium glycinate or malate (300–400 mg daily) reduces prostaglandin production and uterine muscle tension, directly addressing cramping. It also supports phase 2 of liver detoxification and helps regulate blood sugar. Most women are significantly deficient. Start at 100–200 mg and increase gradually.
- Omega-3 fatty acids: High-quality fish oil providing 2–3 g of combined EPA and DHA daily reduces the pro-inflammatory prostaglandins (PGE2) responsible for cramping and heavy flow, and promotes production of anti-inflammatory prostaglandins instead. This is one of the most impactful supplements for period pain of any kind.
- Vitamin D: Vitamin D has significant immune-modulating and anti-inflammatory effects. Deficiency is associated with worse outcomes in estrogen-driven uterine conditions. Get your levels tested; aim for 50–80 ng/mL. Many women require 2,000–5,000 IU daily to reach and maintain this range.
- Curcumin: The active compound in turmeric has potent anti-inflammatory and anti-estrogenic effects — it supports liver estrogen metabolism and directly targets the inflammatory signaling within uterine tissue. Use a high-bioavailability form (with piperine or in a phospholipid complex). Start at 200 mg twice daily and work up to 500 mg twice daily.
- Vitamin E: Has anti-inflammatory and antioxidant effects relevant to uterine tissue, and there is some evidence that it can reduce menstrual pain by inhibiting prostaglandin production. Look for a mixed-tocopherol form. 400 IU daily around menstruation is a common starting point.
- Resveratrol: Emerging research is investigating resveratrol — a polyphenol found in grapes, berries, and Japanese knotweed — as a potential tool for reducing uterine inflammation in adenomyosis and endometriosis. Early studies suggest it may inhibit the proliferation of adenomyotic tissue and reduce inflammation at the endometrial-myometrial junction. While the human evidence base is still developing, the anti-inflammatory and anti-estrogenic mechanism makes it a reasonable addition to a comprehensive protocol. A typical dose used in research is 500–1000 mg daily.
Not sure where to start with your symptoms?
Take the free Hormone Health Assessment to get a personalized protocol based on your specific cycle symptoms and health history. It takes a few minutes and gives you a clear, prioritized starting point.
Take the Free Assessment →Medical Options for Adenomyosis
Natural approaches address the hormonal and inflammatory environment driving adenomyosis and can significantly reduce symptoms. But they do not eliminate adenomyotic tissue. Depending on how severe your symptoms are and what stage of life you are in, medical options may be appropriate — often working best alongside a comprehensive natural protocol rather than instead of one.
The Mirena IUD
The levonorgestrel-releasing intrauterine device (Mirena IUD) delivers a small amount of progestin directly to the uterus, which thins the uterine lining and can dramatically reduce or even stop menstrual bleeding. For many women with adenomyosis, the Mirena is the most effective non-surgical option for managing heavy periods and cramping. It does not treat the underlying adenomyosis, but it can provide meaningful, localized symptom relief. Effects are typically seen within three to six months of insertion, and the device lasts up to eight years.
GnRH agonists
GnRH (gonadotropin-releasing hormone) agonists — such as leuprolide (Lupron) — work by dramatically suppressing estrogen production, effectively inducing a temporary, medically managed menopausal state. Because adenomyosis is estrogen-driven, this can cause symptoms to recede significantly. However, the side effects of induced menopause (hot flashes, bone density loss, mood changes, vaginal dryness) make long-term use impractical. GnRH agonists are generally used for three to six months, sometimes to shrink the uterus before surgery or to provide a window of symptom relief. Symptoms typically return when the medication is stopped and estrogen levels normalize.
Hysterectomy
Hysterectomy — surgical removal of the uterus — is the only definitive treatment for adenomyosis. Because the adenomyotic tissue is embedded throughout the uterine muscle, there is no way to surgically remove just the affected tissue while preserving the uterus (unlike fibroids, which can sometimes be removed individually). For women who have completed their families and whose symptoms are severe and unmanageable by other means, hysterectomy can be genuinely life-changing. It should, however, be considered only after all other options have been fully explored — it is a major surgery with its own recovery and long-term considerations.
The Adenomyosis-Endometriosis Overlap
It is worth reiterating: many women have both adenomyosis and endometriosis simultaneously. Research suggests that around 20 percent of women with endometriosis also have adenomyosis, and the rate among women with uterine fibroids is even higher. If you have a confirmed endometriosis diagnosis and your symptoms — particularly your heavy periods or pelvic pain — seem worse than your endometriosis staging alone would explain, adenomyosis is a reasonable thing to investigate with targeted imaging. The protocols overlap significantly: both conditions benefit from anti-inflammatory nutrition, estrogen dominance support, targeted supplements, and castor oil packs. But adenomyosis has a heavier bleeding component that may warrant additional interventions — both natural (like higher-dose magnesium, vitamin E, and omega-3s targeted at prostaglandin reduction) and medical (like the Mirena IUD).
If you have adenomyosis and suspect you may also have endometriosis, seeking evaluation from a gynecologist with specific expertise in endometriosis is worthwhile. The two conditions together require a more comprehensive diagnostic and management approach than either condition alone.