You've heard it before: "You need to reduce your stress." And like most women I work with, you've probably smiled, nodded, and thought — sure, but how, and what does that even mean for my hormones?
Here's what that advice almost always leaves out: the specific biological chain of events connecting your stress response to your menstrual cycle. Because it is not abstract. Stress suppresses ovulation. It blocks progesterone receptors. It siphons off the raw material your body needs to make sex hormones. And it does all of this through well-mapped, reproducible mechanisms — mechanisms your doctor may not have explained to you, but that are absolutely central to why your period is late, why your PMS has gotten unbearable, or why your cycle seems to have disappeared altogether.
This article is going to give you the full picture: the biology, the three types of stress that disrupt cycles, the specific ways your period changes under stress, and — importantly — what you can actually do about it.
The HPA–HPO Axis Connection: Why Your Brain Links Stress to Your Cycle
To understand why stress wrecks your period, you need to understand two axes that work together — or, under chronic stress, work against each other.
The HPA axis (hypothalamic-pituitary-adrenal) is your stress response system. When your brain perceives a threat — any threat — the hypothalamus fires corticotropin-releasing hormone (CRH), which signals the pituitary to release ACTH, which tells the adrenal glands to produce cortisol. The whole cascade happens within seconds.
The HPO axis (hypothalamic-pituitary-ovarian) is your reproductive system. The same hypothalamus that fires the stress signal also releases GnRH (gonadotropin-releasing hormone), which signals the pituitary to release FSH and LH — the two hormones that tell your ovaries to develop follicles, produce estrogen, trigger ovulation, and make progesterone.
The critical insight here is that both axes share the same command center: the hypothalamus. And when the HPA axis is activated — when your body is in a stress state — the hypothalamus receives a clear biological signal to deprioritize reproduction. It does not distinguish between a lion chasing you through the savanna and a relentless work deadline. All it knows is: danger is present. This is not a good time to grow a baby.
This is not a malfunction. It is a deeply intelligent, ancient survival mechanism. But in a world of chronic, unrelenting stress — what my colleague Dr. Libby Weaver aptly called "Rushing Woman's Syndrome" — that protective mechanism never fully turns off. And that is where the damage to your cycle begins.
The Three Mechanisms: How Cortisol Directly Disrupts Your Hormones
Stress affects your cycle through three distinct, overlapping mechanisms. Understanding each one helps you see why the effects are so pervasive.
Mechanism 1: Cortisol Suppresses GnRH — and Takes Down the Whole Cascade
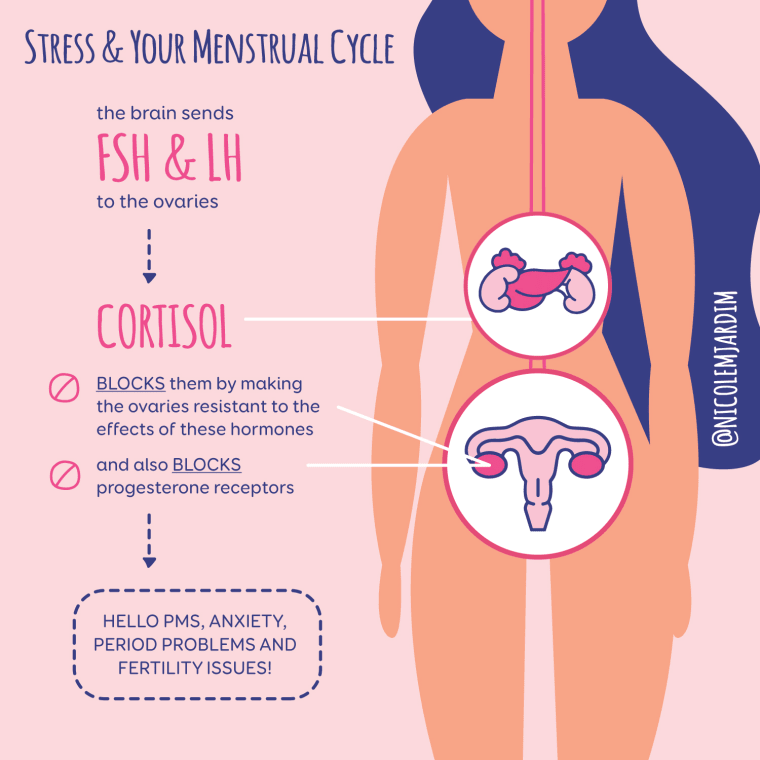
The most direct route: cortisol has a dampening effect on the hypothalamus's ability to release GnRH. Less GnRH means less FSH and LH from the pituitary. Less FSH means follicles in your ovaries don't develop properly. Less LH means the ovulation trigger never fires.
Cortisol also directly inhibits FSH and LH production from the pituitary — a second strike on the same cascade. And if by some miracle enough LH does reach the ovaries, cortisol receptors on the ovarian surface, follicles, and corpus luteum mean that high cortisol can make the ovaries resistant to LH's signal, so estrogen doesn't surge normally and ovulation is still disrupted.
This is a triple blockade: at the hypothalamus, at the pituitary, and at the ovary itself.
Mechanism 2: Pregnenolone Steal — Your Body Robs Your Sex Hormones to Make Cortisol
All of your steroid hormones — cortisol, progesterone, estrogen, testosterone, DHEA — are manufactured from the same starting material: cholesterol, which is first converted into pregnenolone, often called the "mother hormone."
Pregnenolone can go down two main pathways: it can become DHEA and then the sex hormones (progesterone, estrogen, testosterone), or it can become cortisol. In a body under chronic stress, there is enormous demand for cortisol production. Your body responds by directing more and more pregnenolone toward the cortisol pathway — leaving less available for sex hormone synthesis.
Think of pregnenolone as a limited budget. When cortisol becomes the emergency priority, the reproductive hormone department gets its funding cut. Progesterone, estrogen, and testosterone production all suffer as a result.
This is why women under sustained high stress often develop low progesterone, irregular estrogen, and even reduced libido — not because anything is "broken" with their ovaries, but because the raw material has been redirected upstream.
Mechanism 3: Cortisol Blocks Progesterone Receptors
Even when your body manages to produce progesterone, high cortisol can render it functionally useless through a process called competitive inhibition. Cortisol and progesterone have structurally similar hormone receptors, which means cortisol can bind to progesterone receptors — essentially occupying the lock so that the progesterone key can't get in.
The result mimics a progesterone deficiency, even if blood levels of progesterone look normal. You may experience breast tenderness, anxiety and irritability in the second half of your cycle, disrupted sleep before your period, acne, and spotting. And because progesterone is the hormone that converts in the brain to the calming neurosteroid allopregnanolone — which enhances GABA, the brain's primary inhibitory neurotransmitter — this receptor blockade can also amplify PMDD and premenstrual mood symptoms significantly.
The Three Types of Stress That Affect Your Cycle
One of the most important things I teach my clients is that their body cannot tell the difference between types of stress. From a hormonal standpoint, your HPA axis responds to all of the following with the same cortisol cascade.
1. Psychological Stress
This is the stress most people think of: relationship conflict, work pressure, financial worry, loss, trauma. Chronic psychological stress — including early-life trauma, which can fundamentally alter HPA axis sensitivity — is one of the most potent suppressors of ovulation. Women with a history of childhood trauma often have a more reactive stress response in adulthood, meaning their HPA axis fires more easily and takes longer to return to baseline.
2. Physical Stress
Physical stressors are frequently overlooked but are equally powerful in their hormonal effects. These include:
- Chronic under-eating or very low calorie intake — the body reads this as famine and halts reproduction accordingly
- Over-exercising or overtraining — high-intensity training without adequate recovery and nutrition is a major physical stressor that directly suppresses ovulation
- Illness, surgery, and infection — acute physical stressors like the flu, a broken bone, or a gut infection activate the HPA axis intensely
- Chronic illness — conditions like autoimmune disease, Lyme disease, or persistent viral infections (like Epstein-Barr) keep the stress response in a chronic low-grade activation state
- Gut dysfunction — leaky gut, gut infections, and microbiome imbalance are internal physical stressors that continuously activate cortisol production
- Excessive caffeine consumption — caffeine directly stimulates the adrenal glands to produce cortisol, compounding the overall stress load
3. Perceived Stress
This third category is perhaps the most underappreciated. Your nervous system responds not just to what is actually happening, but to how it interprets what is happening. A situation that triggers a full cortisol response in one person may cause only mild activation in another, depending on their stress resilience, nervous system tone, and history.
This is why two women can live through similar life circumstances and have completely different hormonal outcomes. It's not weakness or strength — it's nervous system biology. The interpretation of threat matters as much as the actual stressor. This is also why nervous system regulation work — not just stress reduction — is such a central part of healing cycle disruptions.
Acute vs. Chronic Stress: Why Duration Matters
Not all cortisol is harmful. Acute stress — a short-term, time-limited activation of the HPA axis — is not only normal but beneficial. It sharpens focus, provides energy for the task at hand, and resolves cleanly once the stressor passes. Your cycle may experience a single delayed ovulation after an unusually stressful week, and then return to normal the following month.
Chronic stress is a different animal entirely. When the HPA axis is chronically activated, cortisol dysregulation begins to shift. In early stages, cortisol is chronically elevated — this is when sleep problems, weight gain around the abdomen, blood sugar swings, and cycle irregularity typically emerge. Over time, as the system becomes increasingly exhausted, cortisol patterns can become flatlined — low from morning to night — which presents differently but is equally disruptive to hormonal health. This is what used to be loosely called "adrenal fatigue" and is now more accurately termed HPA axis dysfunction.
Chronic stress also dysregulates melatonin, which is far more than a sleep hormone — melatonin receptors on the ovaries mean that circadian disruption directly affects ovarian function and follicle health. Women who do shift work, for instance, consistently show longer cycles, heavier periods, and greater fertility challenges, driven in part by disrupted melatonin and cortisol rhythms.
How Stress Specifically Changes Your Cycle
The downstream effects of HPA–HPO disruption are not random. They follow a predictable pattern, though different women experience them at different intensities.
Delayed Ovulation and Longer Cycles
The most common and early sign of stress-related cycle disruption is ovulation happening later than usual. Since your period arrives roughly 12–16 days after ovulation (the luteal phase), a late ovulation means a late period. Many women assume they have a "28-day cycle" but, under stress, find their cycle stretching to 35, 40, or even more days. The luteal phase length stays relatively fixed; it's the follicular phase (the time from your period to ovulation) that expands under stress.
Anovulatory Cycles
When stress is severe enough, ovulation may not occur at all. Anovulatory cycles can still produce bleeding — sometimes heavy bleeding — because estrogen continues to build up the uterine lining without the progesterone production that ovulation would have triggered. This "breakthrough bleed" is often mistaken for a normal period. But without ovulation, there is no progesterone surge, and the downstream hormonal effects are significant.
Short Luteal Phase and Low Progesterone
Even when ovulation does occur, chronic stress impairs the quality of the corpus luteum — the temporary gland formed after the egg is released, which is responsible for producing progesterone. A compromised corpus luteum means less progesterone, which shortens the luteal phase (fewer than 10 days is considered short), can cause spotting before your period, and creates the hormonal environment for worsened PMS, mood instability, and difficulty maintaining a pregnancy in the early weeks.
Late or Missed Periods
Both delayed ovulation and anovulatory cycles push your period later or prevent it entirely. A single missed period after a significant stressor is common and usually self-resolving. Repeated missed periods are a signal that the stress load is chronically exceeding your body's capacity to maintain reproductive function.
Heavier or Lighter Periods
The hormonal imbalances created by stress — particularly the progesterone deficit — affect uterine lining development. Low progesterone relative to estrogen can produce a thicker, less organized lining that results in heavier, longer, or more crampy periods. Anovulatory bleeding in particular can be erratic — sometimes very heavy, sometimes very light.
Worsened PMS and PMDD
The connection between stress and PMDD is now well-established in the research. Women with PMDD show a blunted cortisol response to stress in the late luteal phase — meaning their HPA axis is less able to adapt and regulate when faced with sudden challenges in the week or two before their period. The cortisol-progesterone receptor competition described above is especially impactful during the luteal phase, when progesterone levels should be at their highest. When cortisol is occupying progesterone receptors, the calming, GABA-enhancing effects of progesterone cannot be felt — and the result is the anxiety, rage, depression, and overwhelm characteristic of severe PMS and PMDD.
Hypothalamic Amenorrhea
At the severe end of the spectrum, the combination of high psychological stress, insufficient caloric intake, and excessive exercise can suppress the HPO axis so completely that periods stop altogether. This is called hypothalamic amenorrhea (HA), and it's the body's most extreme protection mechanism — a full pause on reproductive function because conditions are deemed too dangerous for a potential pregnancy. HA is not just a fertility issue; the loss of estrogen and progesterone it creates accelerates bone density loss and affects cardiovascular health.
Tracking Clues: How to Know If Stress Is Behind Your Cycle Changes
If you track your cycle — especially with basal body temperature (BBT) and cervical mucus observation — stress disruption leaves recognizable fingerprints:
- Your period is late, but your luteal phase is the same length as usual — this points to delayed ovulation, likely stress-driven
- Your temperature rise never clearly happens — this suggests an anovulatory cycle
- Luteal phase is shorter than 10 days — low progesterone, often connected to HPA axis stress
- Mid-cycle spotting or pre-period spotting — estrogen surges or progesterone drops, both influenced by cortisol levels
- PMS worsens during stressful periods — the cortisol-progesterone receptor competition at work
- Cycles that were regular become irregular during a high-stress chapter of life — the most telling pattern of all
Get your personalized hormonal health protocol
Take the free Hormone Health Assessment — 30 questions about your cycle, symptoms, and lifestyle — and receive a tailored action plan built for your body.
Take the Free Assessment →What to Do: A Protocol for Healing a Stress-Disrupted Cycle
The goal here is not to eliminate stress — that is neither possible nor desirable. The goal is to build enough resilience in your HPA axis and nervous system that normal life stressors stop triggering a hormonal cascade. Here is how I approach this with my clients.
1. Heal the HPA Axis from the Ground Up
Sleep is non-negotiable. Cortisol and melatonin operate in direct rhythm with each other — cortisol should peak in the morning and fall at night, melatonin does the inverse. Disrupted sleep is both a symptom and a driver of HPA axis dysfunction. Aim for 7–9 hours of consistent, dark, screen-free sleep, with a consistent bedtime that allows melatonin to rise naturally.
Blood sugar stability is foundational. Every blood sugar spike and crash sends a stress signal to the HPA axis and triggers a cortisol release. Eating a protein-rich breakfast within 1–2 hours of waking, avoiding long gaps between meals, and pairing any carbohydrates with protein and fat all reduce the blood sugar-driven cortisol load. This is one of the most direct and underestimated interventions for HPA axis healing.
Adaptogens are herbs that specifically support the body's stress resilience and normalize HPA axis function. The most well-researched for cycle-related HPA support include:
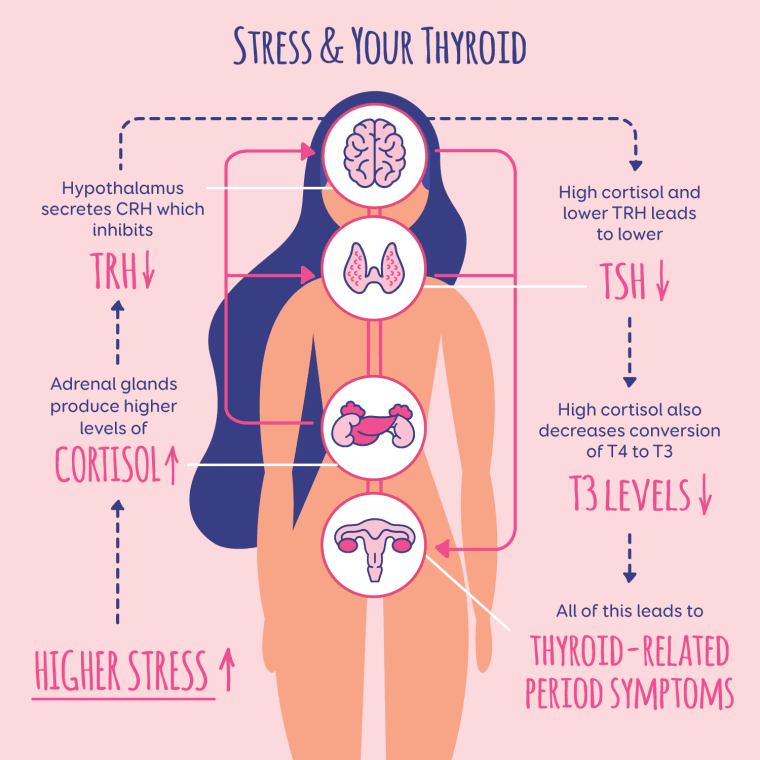
- Ashwagandha — reduces cortisol levels, improves thyroid function, supports progesterone production. Most people do well taking it in the morning; if it's too stimulating, take it before bed instead.
- Rhodiola rosea — improves stress resilience and reduces fatigue without overstimulating the adrenals. Best taken in the morning.
- Eleuthero (Siberian ginseng) — a gentle adaptogen that builds long-term adrenal resilience and supports the immune system under stress.
- Holy basil (tulsi) — calming adaptogen, particularly useful taken in the evening to support cortisol lowering and sleep.
2. Regulate the Nervous System Directly
Adaptogens and diet help the HPA axis over weeks and months. But your nervous system needs real-time downregulation — practices that activate the parasympathetic "rest and digest" state and counteract the chronic sympathetic dominance that stress creates.
Vagus nerve activation is one of the most direct routes. The vagus nerve is the primary driver of the parasympathetic nervous system, and its tone directly predicts how well your body recovers from stress. Practices that improve vagal tone include:
- Deep diaphragmatic breathing with extended exhales — breathing in for 4 counts, holding for 2, exhaling for 6 activates the vagus nerve and lowers heart rate within minutes
- Box breathing — inhale 4, hold 4, exhale 4, hold 4 — particularly effective for acute stress states
- Cold exposure — splashing cold water on your face or ending a shower with 30–60 seconds of cold triggers the dive reflex and strong vagal activation
- Gargling, humming, and singing — these directly stimulate the vagus nerve through vibration of the vocal cords
- Laughter and positive social connection — women uniquely benefit from the "tend and befriend" response to stress, which releases oxytocin and downregulates the HPA axis
Yoga nidra (non-sleep deep rest) has substantial evidence for lowering cortisol and cortisol markers, making it one of the most powerful nervous system reset tools available — and it only requires lying still for 20–30 minutes. HRV training using a wearable device (Oura Ring, Garmin, Whoop, or Apple Watch) lets you track your heart rate variability — a direct measure of vagal tone — so you can objectively see how your nervous system is recovering and which practices help most.
3. Key Supplements for Stress and Cycle Recovery
Magnesium glycinate is my first-line supplement recommendation for virtually every woman with a stress-affected cycle. Magnesium reduces cortisol levels, is required for GABA production in the brain, supports progesterone synthesis, and improves sleep quality. It is depleted by stress, and most people under chronic stress are deficient. Take 300–400mg before bed.
Vitamin C is heavily concentrated in the adrenal glands, which secrete it during the stress response — meaning chronic stress actively depletes vitamin C stores. The adrenals are the organ with the highest vitamin C uptake in the body. Supplementing with 1,000mg per day (divided into two doses) supports adrenal function and cortisol regulation.
B vitamins, especially B5 (pantothenic acid) and B6, are required for multiple steps in adrenal hormone synthesis. Many biochemical pathways for making cortisol, DHEA, and neurotransmitters are B-vitamin dependent. A quality B complex or liver capsule supplement covers this base. Research shows magnesium combined with B6 significantly lowers stress scores.
Omega-3 fatty acids (fish oil) reduce elevated cortisol, protect the brain from the inflammation caused by chronic stress, and support mood stability. Aim for 1,000–2,000mg per day with a minimum of 450mg DHA and 650mg EPA.
4. Reduce the Physical Stress Load
If you are eating in a consistent caloric deficit, exercising intensely every day, or doing both, the physical stress on your HPA axis is enormous — regardless of what is happening psychologically. Your body cannot distinguish "I am undereating for my health" from "there is a famine." The biological response is the same.
This means: eat enough. Aim for protein at every meal (minimum 1g per pound of body weight as a starting point), include adequate fat (the raw material for sex hormone production), and do not skip meals. If you have been under-eating for a long time, work with a practitioner to restore intake gradually.
Pull back on high-intensity exercise if your cycle is disrupted. This is one of the hardest recommendations for many active women to implement, but there is no supplement or adaptogen that can compensate for the HPA activation of daily intense exercise in a body that is already under hormonal stress. Shift toward walking, yoga, strength training at moderate intensity, and Pilates while your system recovers.